



Back to overview – Information
The ilio-sacral joint (SI – joint) or sacrum and iliac joint
(Dr.H.Hiertz)
The SI joint forms the connection between the spine and the pelvis. The bony pelvis forms the foundation on which the rest of the spine is built. The forces generated by the load change when walking are introduced into the pelvis via the hip joint. There are small movements of the pelvis when the load changes. These movements take place in the symphysis and the sacrum and iliac joints. Fig 1

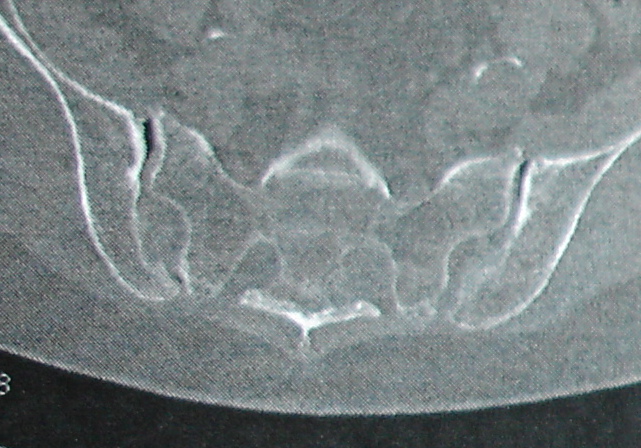
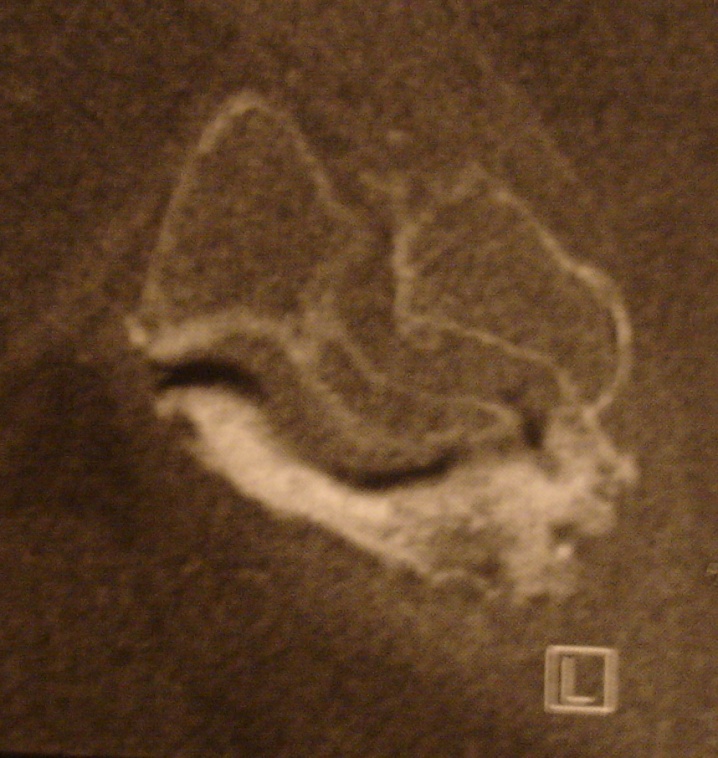
A disturbed position of the spine – profile disturbance – but also deformities and overloading can lead to dysfunction of the SI joint and subsequently to osteoarthritis (wear and tear). Other factors are fractures in the pelvic girdle and congenital malpositions. Fig 2.3
 |
 |
The pain from the SI joint must be differentiated from that caused by wear and tear on the hip joints, but also from problems of the lumbar spine. Sometimes, however, both regions are affected and must therefore be treated or operated at the same time.
The diagnosis is made from the clinic and diagnostic imaging. 25% of all lower back pain comes from the SI joint!
Clinic:
The pain is predominantly present in the lower back, radiating to the thighs and groin, as well as the buttocks, and is clearly intensified when sitting and standing. After a short period of sitting, a relieving position is assumed. In addition, there is usually noticeable tenderness over the SI joint.
Diagnosis:
The diagnosis is made with X-rays of the pelvis and the SI joints and the bony CT of the affected SI joint or an MRI.
Therapie:
First of all, conservative therapy with painkillers, targeted infiltration and therapeutic gymnastics and, on a case-by-case basis, a special corset treatment should always be carried out over a period of several months.
If these measures do not work, a 75% stiffening of the affected SI joint can be achieved. The complication rate of surgical therapy is very low.
Precise planning and clarification are important, especially if stiffening of the lower lumbar spine is necessary. Approx. 45% of the patients who need a stiffening of the SI joint have already had a previous operation on the lumbar spine or the SI joint – one must therefore assume that the SI joint problem was not recognized in many patients. Another risk factor is previous long stiffening of the lumbar spine.
Operation:
With the SI joint operation, a significant improvement can be achieved for many – if one starts from a pain scale where 0 = no pain and 10 = severe pain, the affected persons have an intensity of 8-10 before the operation and up to after the operation 3.
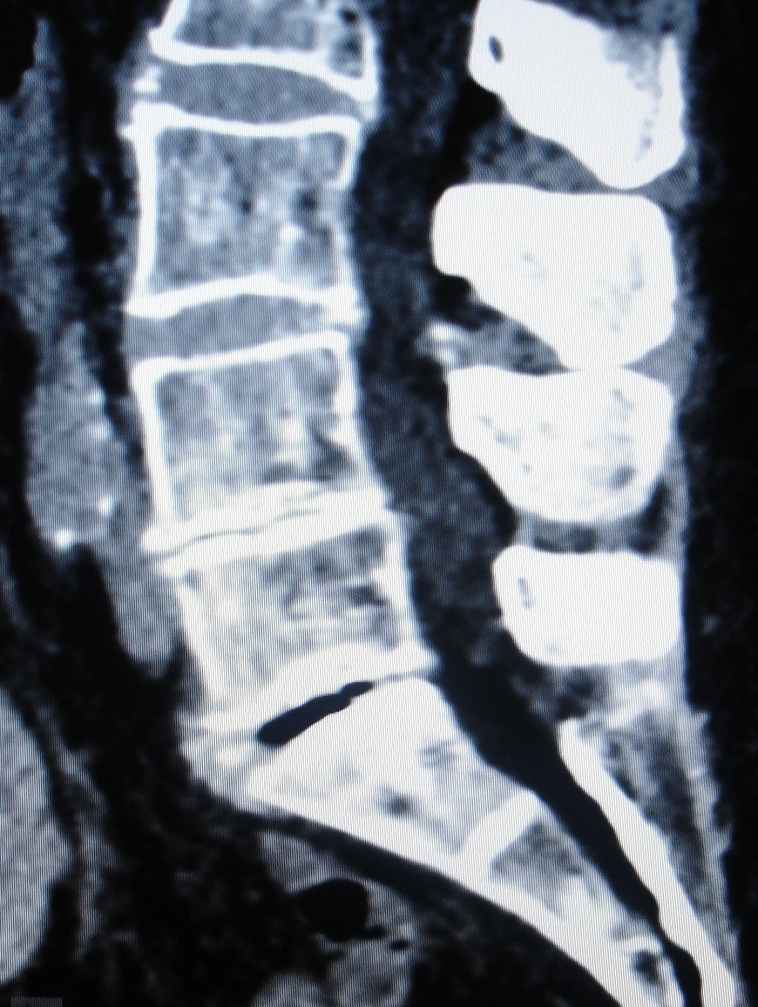
There are various surgical procedures where either an expansion screw (DIANA) and solid bone is inserted into the recess, which has previously been precisely freed from the connective tissue and the nerve endings under a microscope and freshened, but also the surgical procedures coming from the side, which with Screws fix the SI joint. Fig 4.5
|
|
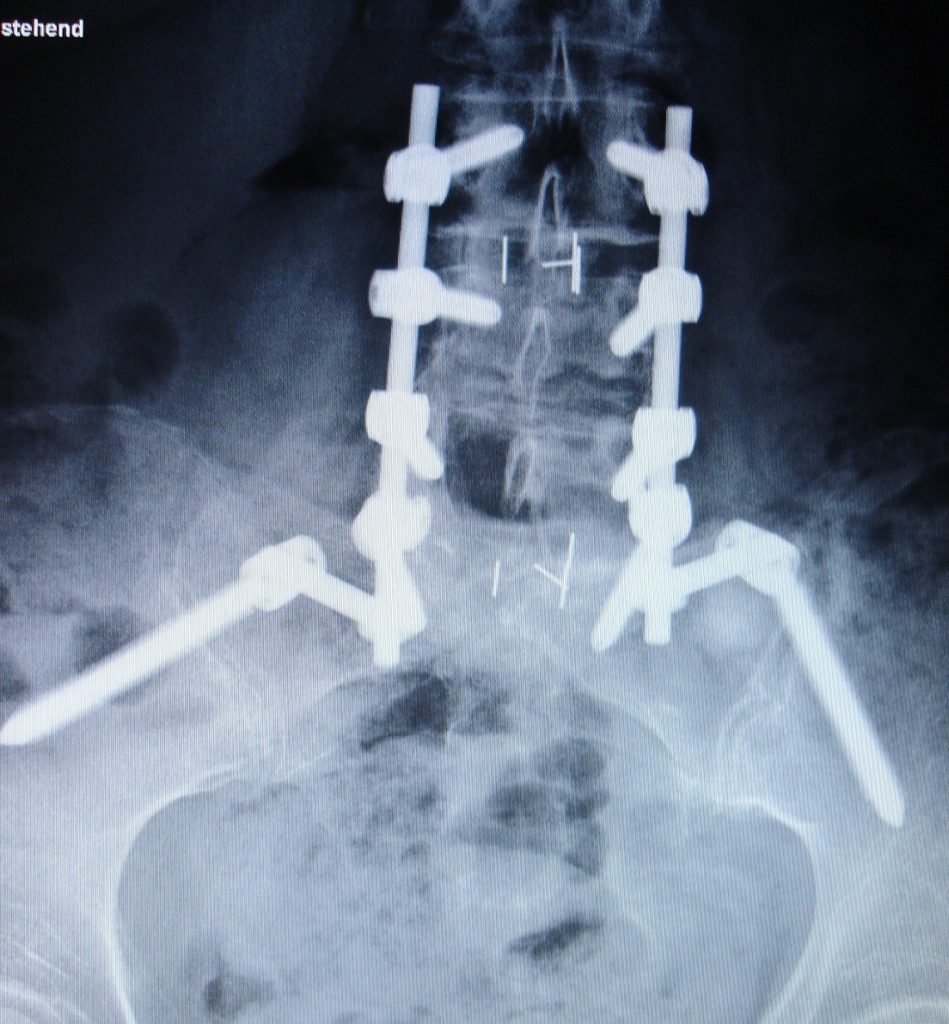
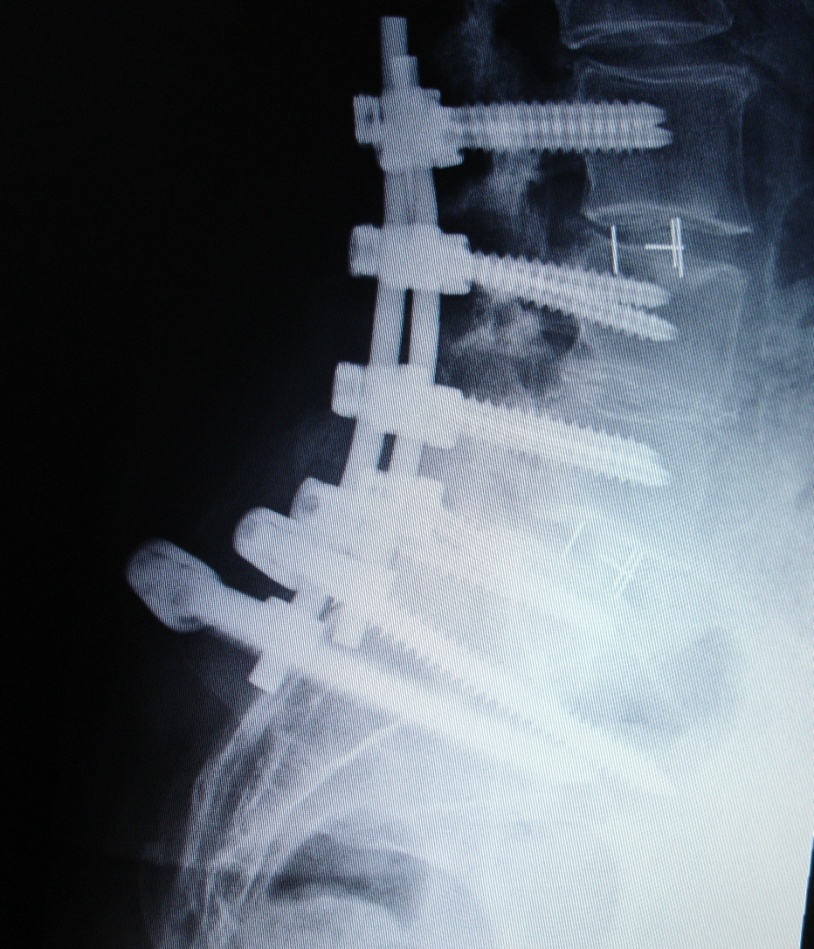
If the SI joint and the lumbar spine have to be operated on, in addition to the lumbar spine stiffening, the SI joint can also be stiffened in the described clearance of the recessus and bone apposition – in this case, however, the lumbar spine is screwed onto the iliac crest (ilium screw) carried out, whereby the bridging takes place. Fig 6,7,8,9,10
 |
|

|
|
|